

Whether you think Obamacare was the worst health care policy of the decade or you join Bernie Sanders in supporting Medicare for All, we can all agree that the current state of the nation’s health care system is untenable and unjust.
Costs are at an all-time high, roughly $11,000 per American, while health outcomes in the U.S. are no better than, or even worse than, other countries like Canada, whose care costs are half of ours.
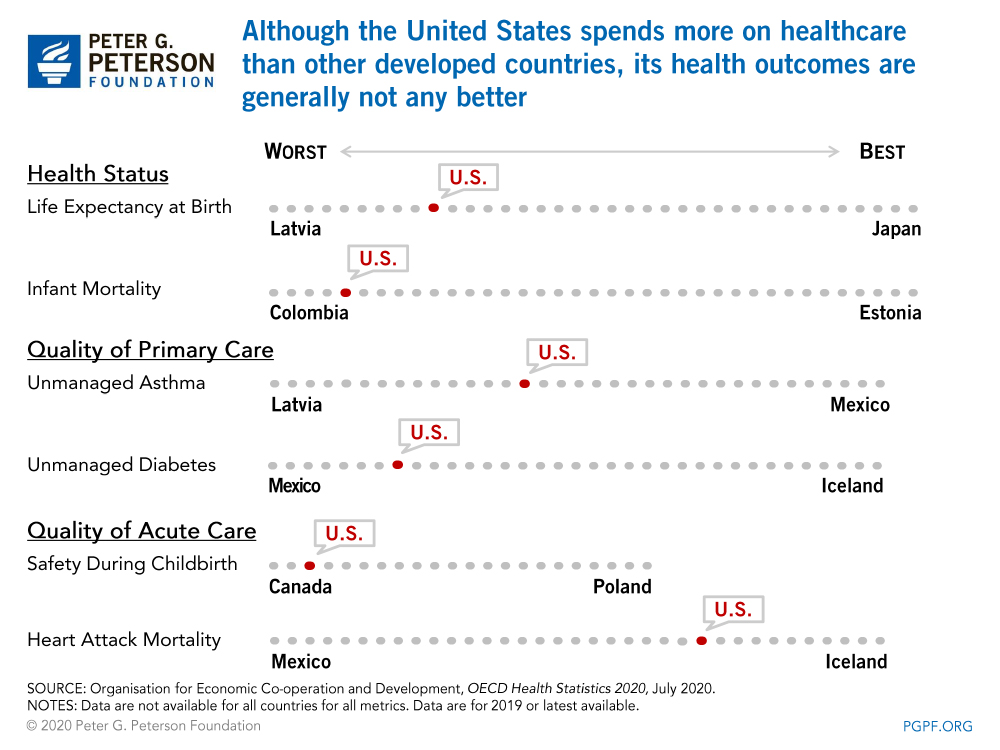
The above graphic from the Peter G. Peterson Foundation illustrates the disparities in U.S. health care costs versus its outcomes.
There have been multiple attempts by the government, at both the state and federal level, to reform our costly system from both sides of the political spectrum. Of them, one of the most flexible, cost-effective, and bipartisan is direct primary care.
Direct primary care (DPC) is an easy and common-sense step to reducing health care costs while improving accessibility. DPC enables patients to enter into a contract directly with their primary care provider, in the form of an affordable monthly or annual fee, in exchange for unlimited access to their doctor and more personalized care. Instead of paying a colossal fee per visit, patients simply pay a recurring fee directly to their practitioner for basic health care, like general visits, physical examinations, and flu shots.
DPC removes third parties and undue barriers, like insurance behemoths and the government, from the doctor-patient relationship.
Maine passed bipartisan legislation cementing the DPC model into state law in 2017.
The beauty of DPC is that it doesn’t codify a one-size-fits-all solution, as do some other health care options, but it just increases the amount of options available to patients. It further strengthens patients’ abilities to find and choose the option that both best fits their needs and is most affordable.
29 states have enacted DPC laws in some form, whether that’s a pilot program or fully fledged, final legislation.
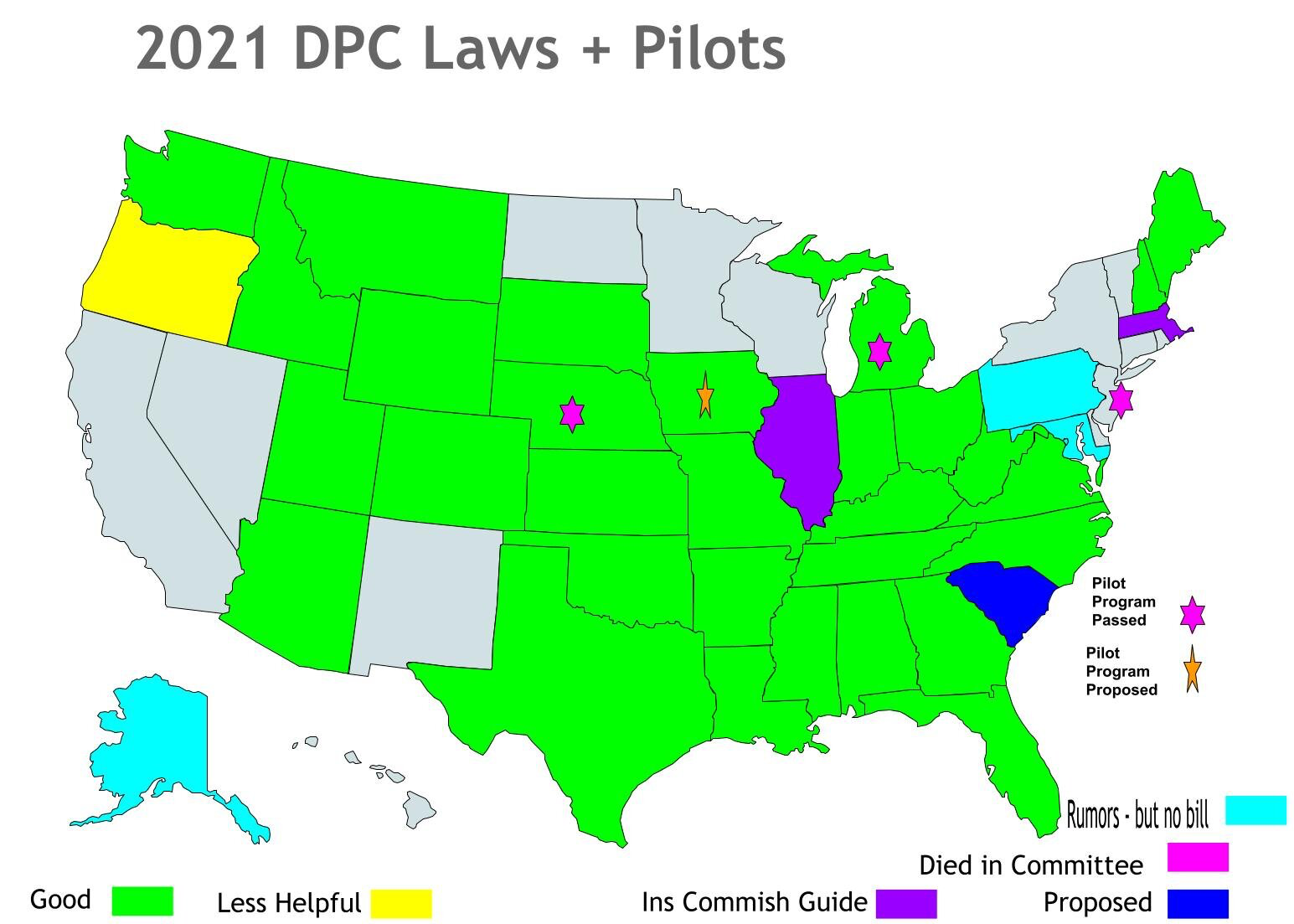
The above image, from DPC Frontier, shows the status of DPC legislation across the country.
Though growing in popularity and recognition across the country, direct primary care legislation has yet to even be introduced in 14 states. Though the model can precede the law, enshrining it into law enables medical practices to engage in DPC if they so choose without the risk of the model being struck down.
A 2016 study from the Annals of Internal Medicine found that doctors spend roughly twice as much time on regulatory and administrative paperwork than they actually do with patients. Such time-consuming work surely contributes to burnout, likely to exacerbate the shortage of doctors in the U.S. that has been forecast over the next two decades. It also encourages them to make patient visits as quick as possible.
DPC helps to mitigate such costly and burdensome administrative work while strengthening the personal relationships between doctor and patient, leading to better, more personalized care.
Direct primary care removes from the equation insurance leviathans who increase costs on families and the maddening red tape that too plagues our current health care system. It gives individuals and families just another option for their health care needs, while lowering costs. It’s a common-sense reform with support on both ends of the political spectrum, and it must continue to be brought up and passed in states across the nation.


